

Why fax-heavy prior authorization intake remains expensive in U.S. healthcare, and how Smart Fax Automator redesigns the workflow
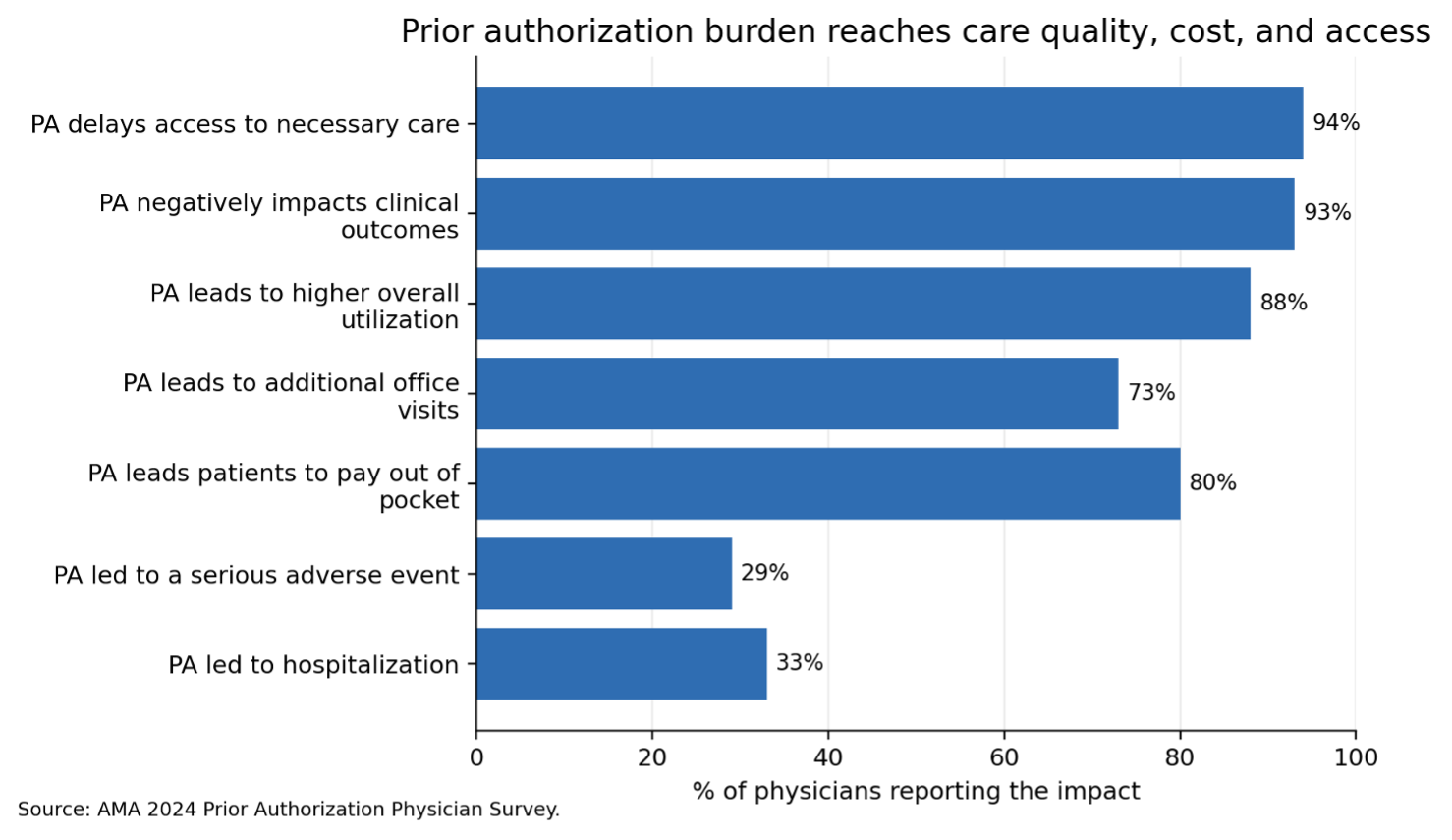
Prior authorization (PA) intake remains one of the most resource-intensive and operationally complex workflows in U.S. healthcare. According to the latest physician survey by the AMA, physicians process nearly 40 prior authorizations per week, with staff spending over 13 hours weekly managing these requests – highlighting the scale of the administrative burden in 2025.
While the industry has made measurable progress in digitization – avoiding an estimated $258 billion in administrative costs through electronic transactions, as highlighted in the 2025 CAQH Index report – a significant opportunity still remains. An additional $21 billion in savings is yet to be realized, largely due to continued reliance on manual and unstructured workflows such as fax.
The process is an operational inconvenience and represents a significant and measurable cost center within utilization management (UM).
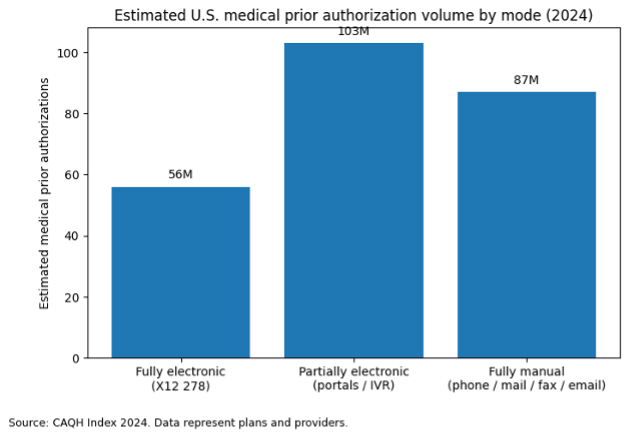
A substantial share of prior authorizations still originates through manual channels, including fax, phone, and email. These workflows are consistently more expensive and time-intensive than electronic alternatives and a contributing factor to care delays, provider abrasion, and suboptimal outcomes.
The core issue is not utilizing fax itself, but what follows. Converting unstructured inputs into decision-ready data requires multiple manual steps like document triaging, data extraction, validation, rework, and routing. Each step introduces friction, cost, and delay.
Industry Check: Why This Problem Still Exists in Healthcare
Healthcare has made steady progress toward digitization, yet prior authorization remains one of the least optimized administrative workflows. Importantly, prior authorization volumes continue to rise year over year.
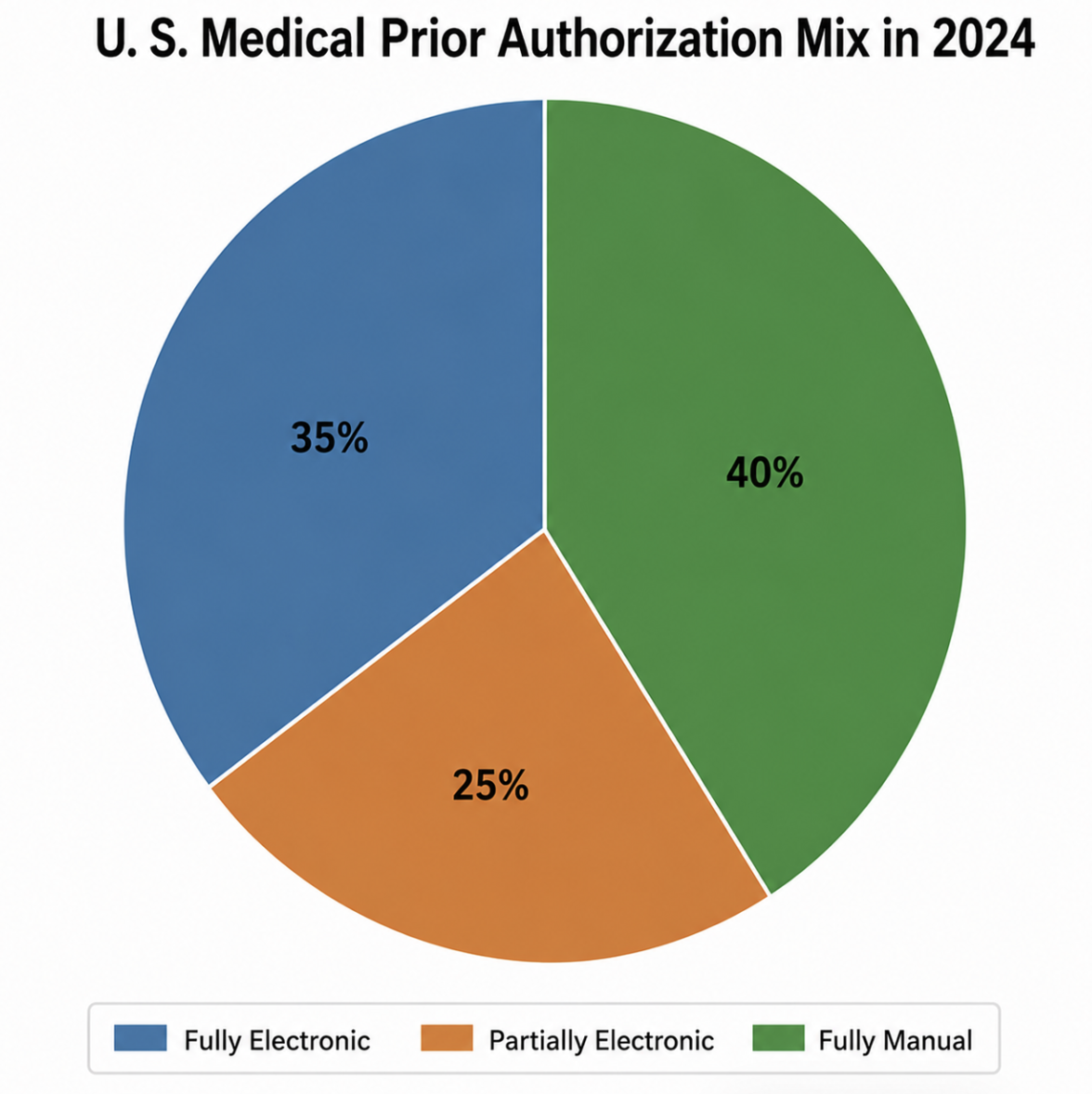
Even in 2025, fewer than one-third of prior authorization transactions were fully electronic. The majority still originate outside structured digital systems, relying on channels such as fax that function as a universal – but inefficient – interoperability layer.
This creates a fundamental disconnect. Providers operate in fragmented environments with varying levels of digital maturity, while payers require structured, validated data to support timely and compliant decision-making.
The result is a persistent handoff gap. Utilization management intake teams are forced to bridge this divide manually, often working through fax packets that contain multiple requests, incomplete information, or inconsistent data. This leads to repetitive data entry into systems such as Jiva and a high dependency on human judgment for basic triaging.
Fax technology remains in use not because it is efficient, but because virtually everyone can access it. This universal compatibility, however, comes with steep costs, making fax one of healthcare's most expensive "necessary complications."
The Real Cost of Manual Fax Intake in Utilization Management
The cost of manual fax processing is often underestimated because it is viewed primarily as a labor issue. In reality, the financial and operational burden extends across multiple layers, each compounding the other.


Why Are Utilization Management Workflows Especially Vulnerable?
Utilization management teams handle some of the highest-stakes administrative work in healthcare — yet they remain heavily dependent on fax-based intake. The problem isn't just the fax itself. It's that intake in utilization management is not a single step, but a multi-stage workflow with multiple failure points.
Each fax must be received, sorted, extracted, validated, routed, reviewed, and entered into a system — manually, repeatedly, and under time pressure. A single error at any stage can delay a prior authorization, trigger a compliance issue, or result in a missed clinical intervention. When volumes scale, so does the risk.
The result: administrative bottlenecks that slow turnaround times, strain staff, and compromise the consistency that utilization management demands.
How ZeOmega's Smart Fax Automator Solves It End-to-End
ZeOmega's Smart Fax Automator replaces this fragmented manual process with a structured, system-driven intake model — purpose-built for utilization management workflows.
Step 1: Secure Intake Orchestration
Fax files land in designated SFTP or DMS locations and are picked up on a scheduled batch cadence, with state tracking (source, picked, completed, error, archived) to prevent duplicates and ensure traceability.
Step 2: OCR/NLP Extraction
Advanced OCR and NLP extract structured data from prior authorization faxes – both typed and handwritten forms, from known templates and unknown documents.
Step 3: Upfront Validation
The system validates critical identifiers before human review: Member ID, Name, DOB, Provider NPI and Clinical Codes (ICD 10, CPT, HCPC). Errors are caught early, preventing downstream rework.
Step 4: Queue Based Exception Handling
Instead of asking users to process every fax from scratch, the system intelligently classifies work:
- Review and Create Episode (clean cases ready for episode creation).
- Review and Confirm Split (faxes containing multiple requests).
- Review Error and Warnings (validation issues requiring correction).
- Review Additional Documents (supporting documents needing attachment).
Step 5: Confidence Led Human Review
Extracted fields are color-coded by AI confidence level (high, medium, low), so reviewers focus attention where the model is least certain. Fields remain editable and confidence scores update after review.
Step 6: Episode Creation and Attachments
Successful cases flow directly into episode creation with data auto-populated. Additional documents attach to members or existing episodes without additional manual steps.
Step 7: Operational Controls and Visibility
Comprehensive dashboard widgets track episode created, member attachments, split reviews, and error processing. Supporting controls include autolocking, queue filtering, sorting, labels, urgent flags, and full audit logging.
The Results
ZeOmega's documented benchmarks show ≥50% reduction in average intake time for configured fax templates and ≥40% for unknown templates, with document-level accuracy ranging from 65% to 80%. These gains reduce administrative overhead while improving turnaround time, consistency, and scalability across the full scope of utilization management operations.
From a performance standpoint, ZeOmega’s documented benchmarks indicate ≥50% average intake-time reduction for configured fax templates and ≥40% for unknown templates, alongside document-level accuracy levels ranging from 65% to 80%. These gains not only reduce administrative overhead but also improve turnaround time, consistency, and scalability across utilization management operations.
ZeOmega’s Smart Fax Automator eliminates inefficiencies through targeted controls.
Reimagining Fax Intake: The Smart Fax Automator Approach
The Smart Fax Automator workflow transforms unstructured fax intake into a structured, decision-ready process, combining automation with targeted human review to improve speed, accuracy, and scalability across utilization management.

The Business Case: From Cost Center to Efficiency Driver
The impact of automation becomes most visible when translated into operational and financial outcomes.
ZeOmega’s Smart Fax Automator demonstrates up to a 50% reduction in intake time for structured templates and at least 40% for unstructured formats, with data extraction accuracy ranging between 65% and 80%.
For high-volume payers processing large volumes of fax-based authorizations, these improvements translate into substantial cost savings, reduced manual workload, and faster turnaround times.
However, the true value extends beyond direct cost reduction. Organizations benefit from lower rework, improved provider experience, faster case creation, and stronger compliance readiness.
More importantly, utilization management teams are able to shift focus from manual data processing to higher-value clinical and decision-support activities.
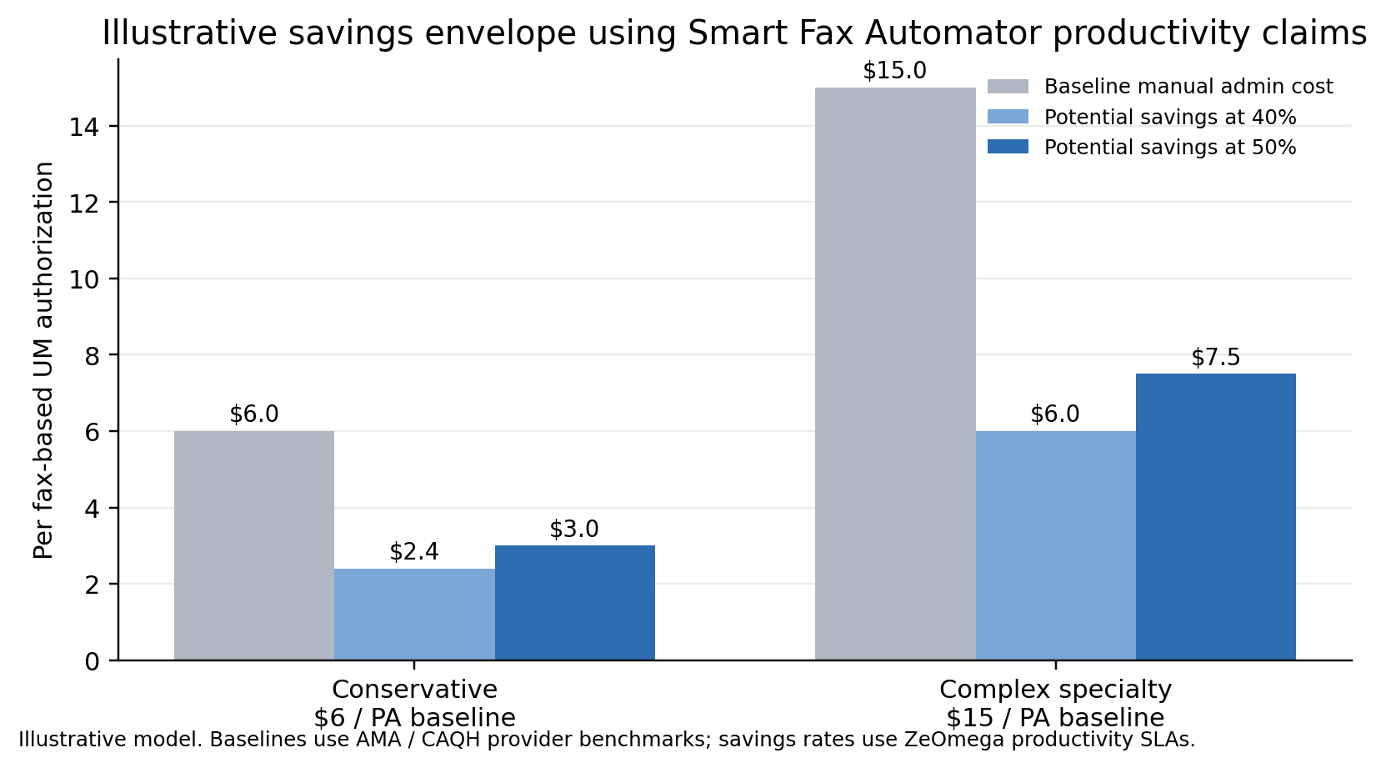
Estimated Annual Savings Opportunity from Automating Fax-Based Utilization Management Intake
These figures exclude secondary benefits that are often material in utilization management: lower rework, faster turnaround, fewer provider callbacks, less time spent searching Jiva for corrections, lower duplicate handling, and better compliance support.
Bottom Line: The Strategic Shift
Manual fax processing is not simply a legacy inconvenience. It is a systemic inefficiency embedded within one of healthcare’s most critical workflows.
The broader industry dynamics are clear. Prior authorization volumes are increasing, regulatory expectations are tightening, and administrative cost pressures continue to grow. At the same time, fax remains deeply embedded in provider workflows.
The question is no longer whether fax will persist. It is whether organizations can afford to continue processing it manually.
ZeOmega’s Smart Fax Automator represents a strategic shift transforming fax intake into a structured, intelligent, and scalable process aligned with the future of utilization management.
To learn more, contact us at sales@zeomega.com or 214.618.9880.
